
Scribe Shield: How CTOs Can Vet HIPAA AI Scribes in 2026
June 01, 2026 / Bryan Reynolds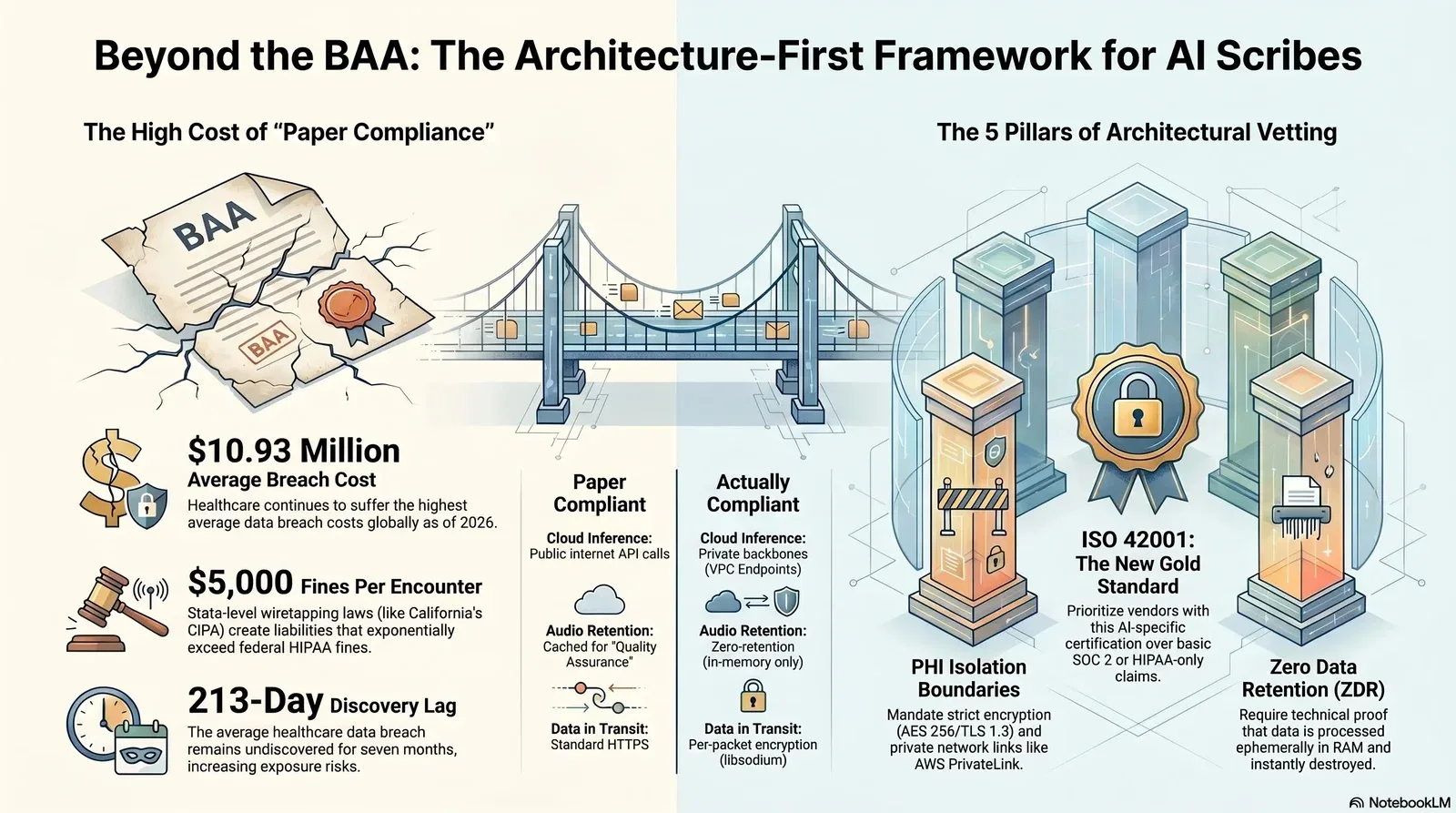
HIPAA-Compliant AI Scribes and Agents: A Healthcare CTO's Vendor Vetting Checklist
The deployment of artificial intelligence in healthcare documentation has definitively transitioned from an experimental pilot phase to mainstream operational dependency. As of early 2026, empirical data indicates a massive adoption spike, with 63% of the physician workforce actively utilizing AI tools, predominantly for voice-based documentation and ambient scribing. Among specialized disciplines, neurologists lead this adoption curve at 64%, followed closely by gastroenterologists and internists at 61% and 60%, respectively. This rapid integration is driven by a measurable reduction in administrative burden, with current AI users reporting up to a 48% decrease in after-hours charting, colloquially known as "pajama time". Consequently, the global market for artificial intelligence in healthcare is projected to reach $51.20 billion in 2026, expanding at a compound annual growth rate (CAGR) of 36.83%, with North America maintaining the largest market share.
However, the proliferation of ambient clinical agents has introduced unprecedented architectural complexities regarding the processing, transmission, and storage of Protected Health Information (PHI). For Chief Technology Officers (CTOs) and Chief Information Security Officers (CISOs) in healthcare organizations, the fundamental challenge is discerning between a HIPAA compliant AI scribe that is merely "compliant on paper" and a vendor whose technical architecture, sub-processor ecosystem, and incident response playbooks can withstand rigorous scrutiny from the Office for Civil Rights (OCR), forensic auditors, and plaintiff attorneys. This is also where a broader, phased enterprise AI implementation plan becomes critical so the scribe is part of a coherent AI roadmap instead of a risky one-off tool.
The financial stakes of misjudging this distinction are severe and escalating. According to IBM's Cost of a Data Breach Report, the healthcare industry continues to suffer the highest average breach costs globally, reaching an unprecedented $10.93 million, with the average breach remaining undiscovered for an astonishing 213 days. Furthermore, the introduction of unvetted generative AI tools into the clinical environment creates severe Shadow AI Risks. For organizations with high levels of unmonitored or "shadow" AI usage, these breaches add an average of $670,000 to the total breach cost compared to organizations with strict AI governance, as these incidents frequently result in widespread exposure of personally identifiable information across multiple unsecured environments. In this hostile threat landscape, treating a signed Business Associate Agreement (BAA) as a substitute for deep architectural vetting is a systemic failure that exposes covered entities to catastrophic regulatory and financial liabilities.
This exhaustive research report provides healthcare technology buyers with a definitive, architecture-first vendor-vetting framework. It systematically deconstructs the legal, architectural, and operational mandates required to securely deploy AI scribes in a modern clinical environment, moving far beyond the baseline checklist of standard compliance frameworks and aligning with a broader strategy for managing Shadow AI risks across the organization.
Why "HIPAA Compliant" is the Wrong Question: The 2026 Enforcement Landscape
The healthcare technology sector relies heavily on the term "HIPAA compliant" as a primary marketing mechanism. However, HIPAA is not a static software certification; it is a regulatory framework governing the behavior, policies, and technical safeguards of organizations handling PHI. A vendor advertising basic compliance on their homepage merely signals a willingness to execute a standard BAA and apply elementary data-at-rest encryption. In the 2026 enforcement environment, this baseline is fundamentally inadequate to protect a covered entity from profound legal and financial exposure.
The OCR Enforcement Paradigm and Business Associate Liability
The Department of Health and Human Services (HHS) Office for Civil Rights (OCR) has shifted its enforcement focus aggressively toward risk analysis failures and supply-chain vulnerabilities. Recent enforcement actions demonstrate a clear, punitive upward trend against organizations that fail to document comprehensive risk analyses or meticulously manage the security posture of their third-party business associates. The regulatory expectation has evolved from merely identifying risks to proving documented remediation efforts and continuous, real-world risk mitigation that fits into a disciplined, DevOps-style governance and monitoring program.
A seminal example of this aggressive posture is the OCR's settlement with MMG Fusion, a healthcare software vendor acting as a business associate. Following an investigation initiated by a complaint regarding an unreported security incident and the subsequent discovery of PHI on the dark web, the OCR found systemic compliance failures. The investigation revealed that malicious actors had infiltrated the vendor's systems, accessing the PHI of approximately 15 million individuals. Crucially, the OCR determined that the vendor failed to conduct an accurate and thorough risk analysis and, catastrophically, failed to execute timely breach notifications to its covered entity clients. While the financial penalty in this specific instance was negotiated down to $10,000 due to the vendor's limited financial standing, the imposition of a stringent, highly monitored three-year Corrective Action Plan (CAP) serves as a stark warning. For a healthcare CTO, the primary takeaway is that an AI scribe vendor's failure to maintain robust internal security postures directly compromises the covered entity's data integrity and operational continuity.
The Emergence of State-Level Privacy and Wiretapping Litigation
Beyond federal HIPAA enforcement, the most immediate existential threat to healthcare organizations deploying ambient AI scribes stems from aggressive state-level privacy, medical confidentiality, and wiretapping legislation. Technical architectures that continuously stream ambient clinical audio to external cloud servers are actively triggering mass, high-stakes litigation that bypasses standard healthcare regulations.
The bellwether case of Washington v. Sutter Health et al. perfectly illustrates this localized vulnerability. In April 2026, a high-profile class-action lawsuit was filed in the U.S. District Court for the Northern District of California against major healthcare providers, alleging severe violations of the California Invasion of Privacy Act (CIPA), the California Confidentiality of Medical Information Act (CMIA), the California Unfair Competition Law, and the Federal Wiretap Act. The complaint specifically targets the deployment of Abridge, an enterprise-grade ambient clinical documentation system, though the underlying legal theories apply to virtually any ambient AI platform.
The plaintiffs allege that microphone-enabled devices deployed in examination rooms captured highly sensitive patient-provider conversations, which were subsequently transmitted to external, third-party cloud servers for processing, transcription, and generative AI model ingestion without explicit, legally sufficient patient consent. Because California operates as an all-party consent state regarding the interception and recording of communications, the plaintiffs are seeking massive statutory damages of $5,000 per recorded encounter. For a medium-to-large health system processing tens of thousands of clinical encounters daily, the cumulative financial exposure under CIPA and CMIA exponentially exceeds maximum federal HIPAA fines. This litigation demonstrates that architectural vetting must evaluate exactly how and where vendor data flows intersect with state wiretapping statutes, regardless of whether a federal BAA has been executed, and why a broader view of how SaaS and AI contracts reshape enterprise risk now matters more than ever.
Navigating Generative AI Notification Mandates
Compounding the legal complexity of ambient recording are state-specific mandates governing the disclosure of artificial intelligence usage. Healthcare organizations operating in or treating patients from jurisdictions with strict AI transparency laws must ensure their vendor deployments allow for seamless compliance.
In California, Assembly Bill (AB) 3030, effective January 1, 2025, requires health facilities, clinics, and physician's offices to explicitly notify patients whenever Generative Artificial Intelligence (GenAI) is utilized to communicate "patient clinical information". The statute meticulously defines the formatting requirements for these notifications based on the medium: written communications require prominent display at the beginning of the text, continuous chat interfaces require persistent display, audio interactions require verbal notification at both the initiation and conclusion of the communication, and video interactions require persistent visual display.
While AB 3030 provides a critical "human review exemption"—stating that communications read and reviewed by a licensed or certified human health care provider are exempt from these specific notification requirements—the operationalization of ambient scribes still frequently triggers broader consent and disclosure requirements regarding the initial audio capture. A healthcare CTO must ensure that the AI scribe's interface and the organization's overarching governance policies are highly synchronized to manage these state-level nuances.
Deconstructing the Business Associate Agreement in 2026
Under the HIPAA Privacy Rule, any artificial intelligence vendor that creates, receives, maintains, or transmits PHI on behalf of a covered entity acts as a Business Associate. Ambient AI scribes that capture live audio, process transcripts, and generate structured clinical notes via large language models (LLMs) inherently and unavoidably fall into this category. Consequently, executing a BAA is a mandatory legal prerequisite prior to transmitting any clinical data to the vendor's cloud architecture.
However, vendor-supplied BAAs are frequently drafted as boilerplate documents designed to minimize the vendor's operational liability while maximizing their rights to exploit processed data. Healthcare CTOs must transition from treating the BAA as a procurement formality to recognizing it as a critical instrument of risk transference, aggressively negotiating its constituent clauses as part of a disciplined service contracts and vendor management strategy.
Critical BAA Clauses for Aggressive Negotiation
The standard vendor BAA must be thoroughly dissected and amended to include strict, highly favorable terms for the covered entity. The most critical areas of negotiation include incident response timelines, liability caps, and secondary data usage rights.
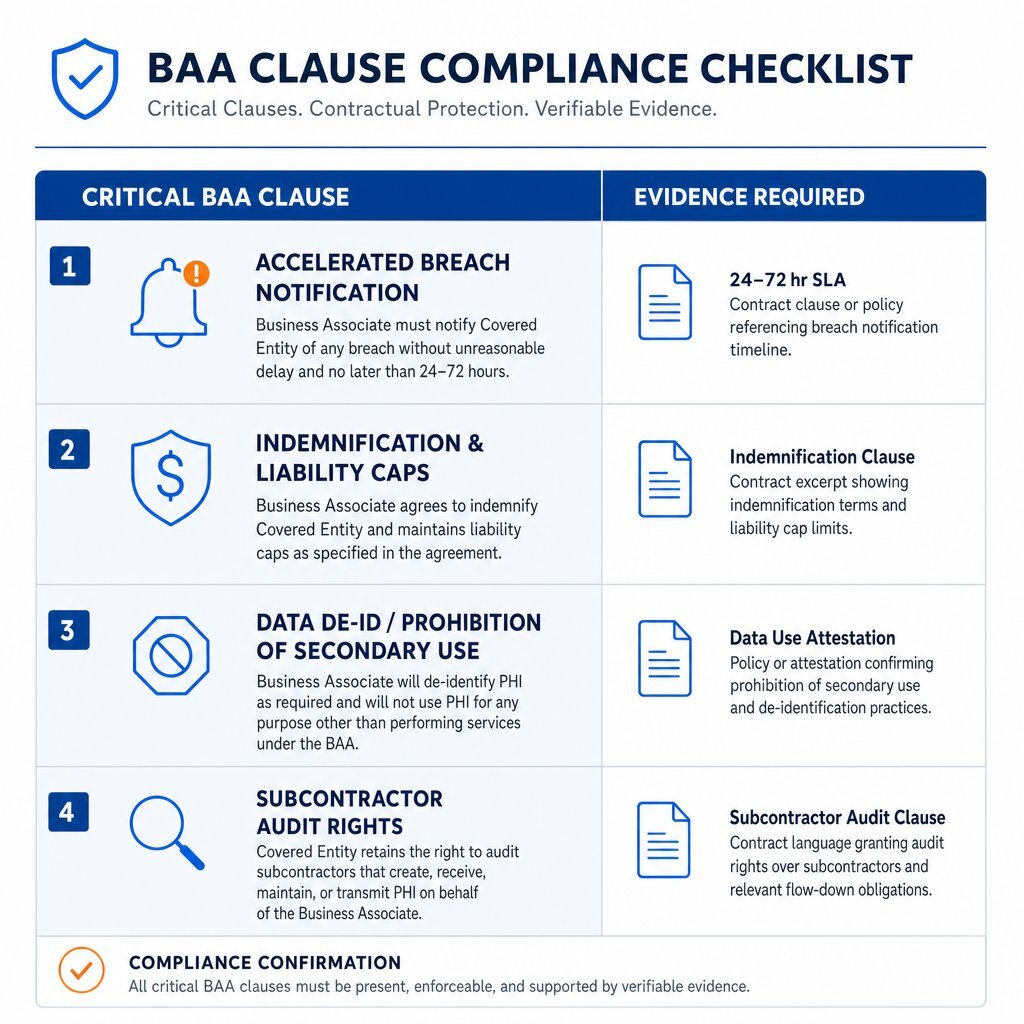
1. Accelerated Breach Notification Timelines (The Incident Response SLA) HIPAA regulations provide a generous allowance, legally permitting a business associate up to 60 days to notify a covered entity following the discovery of a data breach. In the context of a high-velocity AI platform processing thousands of live, highly sensitive clinical encounters simultaneously, a 60-day notification window is a catastrophic vulnerability. By the time the covered entity is notified, the compromised PHI could have been fully exfiltrated, monetized on dark web forums, or ingested into irreversible downstream machine learning pipelines. CTOs must mandate accelerated breach notification Service Level Agreements (SLAs) within the BAA, strictly requiring the vendor to provide formal notification within 24 to 72 hours of a suspected or confirmed security incident. This rapid timeline is an absolute necessity, allowing the covered entity to enact its own incident response playbooks, revoke API access tokens, and mitigate downstream harm to the patient population.
2. Indemnification and Substantial Liability Caps Standard SaaS vendor BAAs often contain mutual indemnification clauses and liability caps that are aggressively restricted to a mere 12 months of paid subscription fees. This is disproportionately inadequate given the multimillion-dollar exposure of a healthcare data breach. Healthcare buyers must negotiate robust, unilateral indemnification provisions that hold the AI vendor financially responsible for OCR fines, class-action settlement costs, and third-party forensic investigation expenses that result directly from the vendor's negligence, architectural failures, or inability to maintain their stated security controls. While vendors will heavily resist lifting liability caps entirely, negotiating carve-outs for gross negligence, intentional misconduct, and specific breaches of confidentiality is critical.
3. Data De-Identification and Prohibition of Secondary Use A highly pervasive and lucrative practice among AI scribe vendors is the inclusion of "secondary use" or "service improvement" clauses within the BAA. These provisions legally permit the vendor to aggregate and de-identify the covered entity's PHI to train their proprietary foundational models, fine-tune algorithms, or develop derivative commercial products. For example, a vendor's terms may state that they have the right to process de-identified data for training internal AI models, asserting that such data no longer constitutes PHI under HIPAA's Safe Harbor de-identification standards. If the healthcare organization's institutional governance policy prohibits the use of patient data for third-party commercial AI model training, the CTO must ensure the BAA explicitly and unambiguously forbids the creation of de-identified datasets for vendor commercialization.
4. Stringent Subcontractor Management and Audit Rights The BAA must legally compel the primary AI vendor to ensure that any downstream sub-processors—such as cloud infrastructure providers, vector database hosts, or third-party LLM inference APIs—are contractually bound by the exact same stringent security and privacy restrictions as the primary vendor. Furthermore, the BAA should grant the covered entity the explicit right to audit the vendor's security infrastructure, demand copies of internal risk assessments, and review independent penetration testing reports on an annual basis. These contractual protections should sit alongside a modern, finance-aware view of AI vendor ROI and risk so legal terms and economics stay aligned.
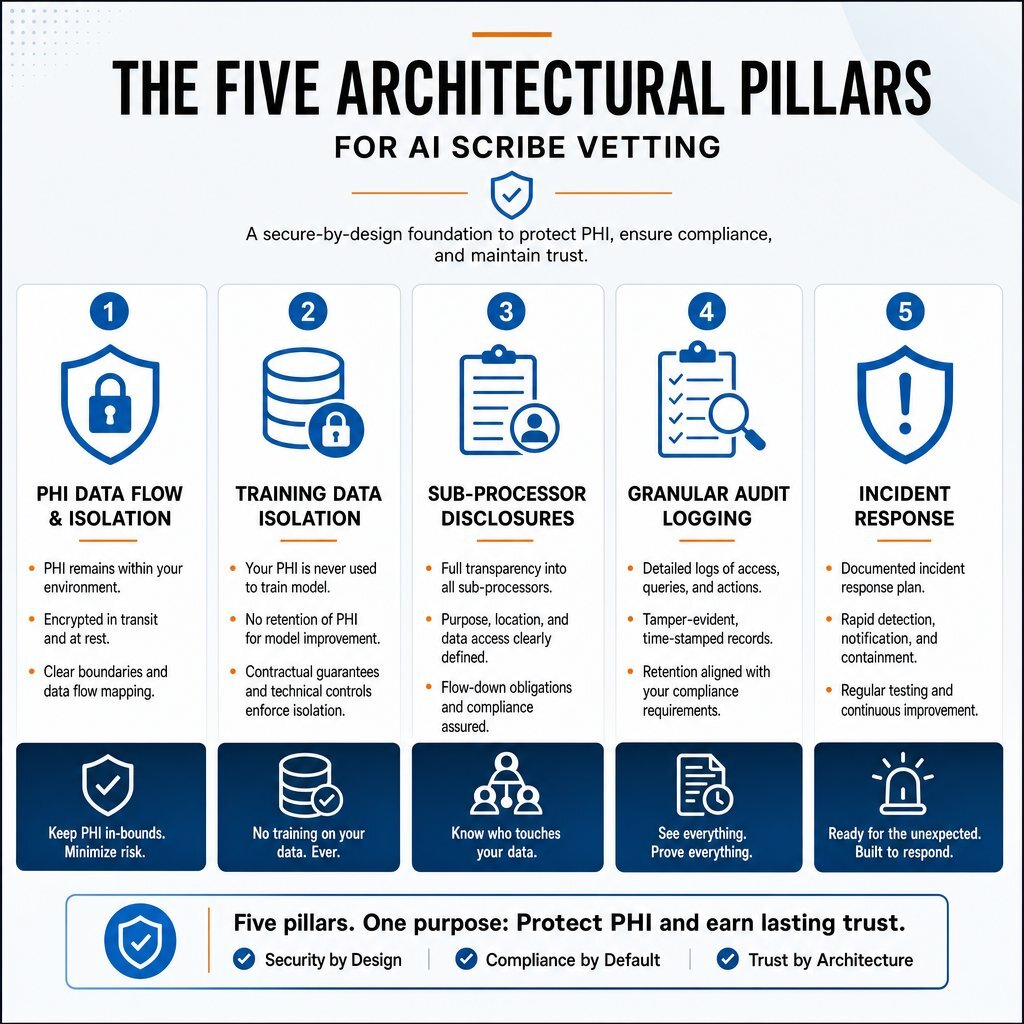
The Five Architectural Questions for a Defensible AI Scribe
A legally sound, aggressively negotiated Business Associate Agreement provides contractual recourse, but it is the underlying technical architecture that provides actual, preventative security. When evaluating an AI scribe vendor, the vetting process must transition from legal document review to deep, uncompromising architectural interrogation. The fundamental gap between a vendor who is "compliant on paper" and one who is architecturally secure is determined by five specific technical pillars, which should plug into your broader AI data infrastructure and governance strategy.
Pillar 1: PHI Data Flow and Strict Isolation Boundaries
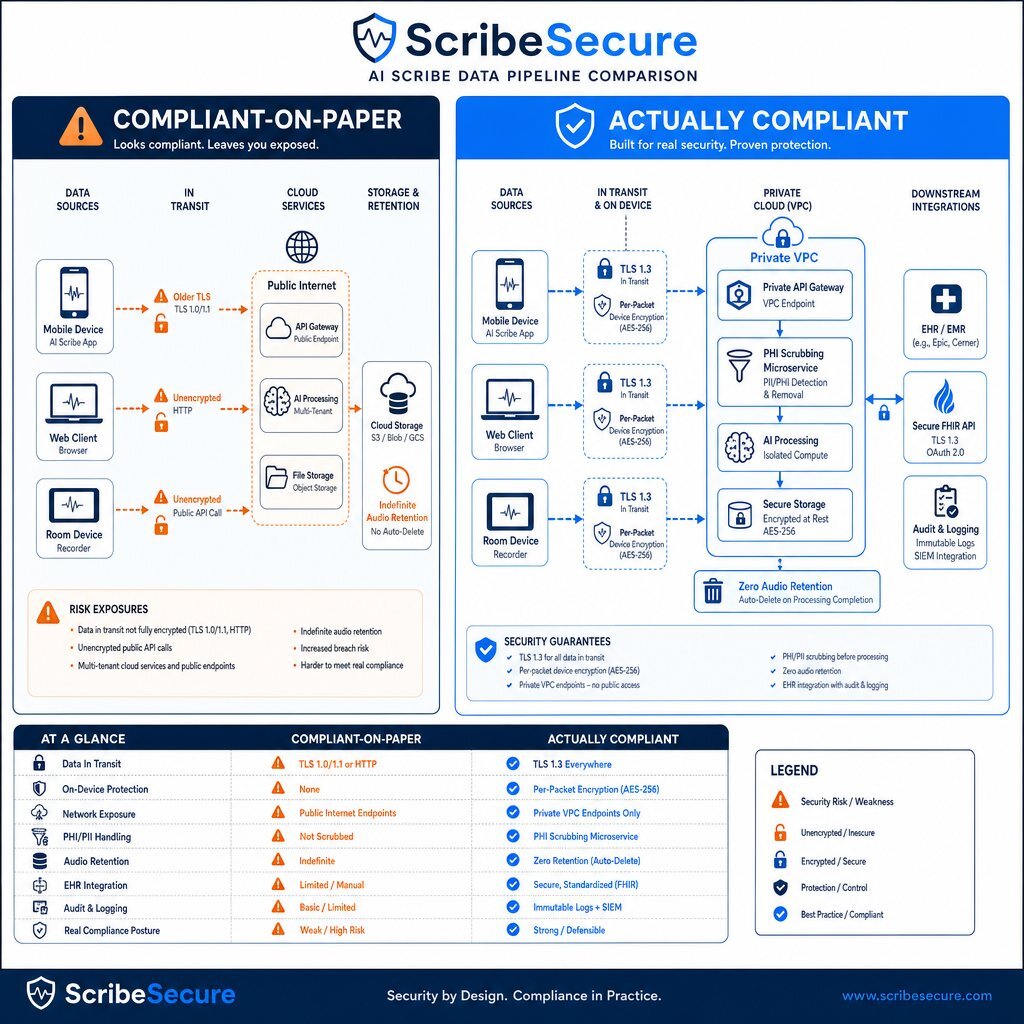
The preliminary step in evaluating an AI clinical agent is demanding a comprehensive, highly detailed data flow diagram. This diagram must explicitly map the entire lifecycle of clinical audio: from the edge capture device (such as a physician's managed mobile phone or a dedicated ambient microphone), through the network transit layer, into the cloud ingestion point, through the transcription and LLM inference engines, and finally back into the Electronic Health Record (EHR) system.
A defensible, genuinely HIPAA-compliant data flow establishes a strict, impenetrable PHI Isolation Boundary. Inside this boundary, every single microservice, compute cluster, database, and ephemeral container is heavily hardened and continuously monitored. Outside this boundary, zero unencrypted PHI should exist under any circumstances.
Architectural Standards to Demand: The vendor must demonstrate end-to-end encryption utilizing modern cryptographic standards. Data must be encrypted at rest utilizing Advanced Encryption Standard (AES) 256-bit encryption. In transit, data must be protected using Transport Layer Security (TLS) 1.2 at an absolute minimum, though TLS 1.3 is strongly preferred and increasingly considered the industry standard.
For edge deployments, particularly mobile applications, audio data should ideally be encrypted per packet directly on the device using advanced protocols such as the libsodium secret stream (XChaCha20 with Poly1305 MAC) before it ever interacts with the network layer. This ensures that even if the mobile device is compromised or network traffic is intercepted, the audio payload remains entirely unreadable. Furthermore, mobile architectures must be designed to decrypt, upload, and instantly delete the audio from the local device memory immediately upon successful synchronization with the cloud backend.
If the vendor's infrastructure is hosted on major public clouds like Amazon Web Services (AWS) or Microsoft Azure, the architecture should heavily utilize Virtual Private Clouds (VPCs). Public-facing endpoints must be protected by an Application Load Balancer (ALB) terminating TLS, situated safely behind a Web Application Firewall (WAF). Crucially, any API calls made to foundational models (e.g., AWS Bedrock, Amazon SageMaker, or Azure OpenAI) must occur via private network links, such as VPC Endpoints or AWS PrivateLink, to guarantee that PHI never traverses the public internet during the inference phase.
| Architectural Feature | "Compliant-on-Paper" Data Flow | "Actually Compliant" Data Flow |
|---|---|---|
| Data in Transit | Standard HTTPS, older TLS 1.0/1.1 accepted. | Strict TLS 1.3 enforcement; per-packet encryption on edge devices (e.g., libsodium). |
| Cloud Inference | Inference calls sent over the public internet to third-party LLM APIs. | Inference calls routed through private backbones (e.g., AWS PrivateLink) with zero internet exposure. |
| Audio Retention | Audio cached indefinitely on mobile devices or cloud storage for "quality assurance." | Audio processed in memory and immediately destroyed post-transcription (Zero-Retention). |
| Boundary Protection | Basic cloud tenant separation. | Strict PHI Isolation Boundaries; external API calls passed through dedicated PHI-scrubbing de-identification microservices. |
Pillar 2: Training Data Isolation and Model Boundaries
The most pervasive and justified fear among healthcare providers regarding AI scribes is the prospect of their patients' highly sensitive clinical narratives being ingested into a foundational model's massive training corpus, potentially surfacing as an output in a completely different context or exposing proprietary medical decision-making algorithms. Vendors frequently make broad, unverified marketing claims asserting, "We never use your data to train our models." CTOs must look past the marketing and demand technical proof of this assertion, understanding that vendors approach data retention with vastly different engineering philosophies.
Architectural Approaches to Data Retention:
- Zero-Retention Architectures: Certain vendors lean heavily into a privacy-first posture, explicitly marketing a "no audio stored by default" capability. In these systems, data is processed ephemerally in random-access memory (RAM) and the original audio file is discarded immediately post-transcription. For instance, platforms like Nabla advertise an absence of default audio storage, though they may offer configurable retention periods (e.g., 14 days) based on the specific needs of privacy-sensitive practices.
- Time-Boxed Retention: Other platforms employ a highly documented, strict retention schedule. Suki AI, for example, dictates that the original audio input and the generated raw transcript are permanently destroyed after 30 days, while the final, structured clinical note is retained for the duration of the service contract to facilitate ongoing EHR integration and historical review.
- Immediate Deletion on Sync: Enterprise tools such as Nuance Dragon Copilot design their mobile applications with aggressive ephemeral storage. Audio recordings are encrypted locally and deleted from the local device immediately after they are successfully uploaded to the cloud. If the device is offline, encrypted recordings are kept locally only until connectivity is restored, uploaded, and then instantly purged.
To rigorously verify training isolation, the CTO must demand the vendor's internal data governance policies and, critically, their API agreements with upstream model providers (e.g., OpenAI, Anthropic, or proprietary cloud hosts). If the vendor utilizes third-party LLMs, they must provide binding documentation proving they are utilizing "Zero Data Retention" (ZDR) enterprise endpoints. This ensures the LLM provider is contractually and technically blocked from retaining the API prompt history for any future model training or telemetry gathering, echoing the architect-led guardrails needed whenever autonomous AI agents touch critical systems.
Pillar 3: Sub-Processor Disclosures and Fourth-Party Risk
Modern generative AI applications are rarely monolithic, self-contained architectures. They are highly complex, interwoven pipelines heavily reliant on an ecosystem of third-party sub-processors for specialized tasks: speech-to-text recognition models, natural language processing sentiment engines, highly optimized vector databases, and foundational LLM inference APIs. A massive, critical vulnerability in the vendor evaluation process is the failure to map these "fourth-party" risks. Understanding Third-Party & Supply Chain Risk is no longer an optional component of IT governance; it is central to surviving an audit.
A recent, comprehensive industry analysis conducted by DataGrail analyzed 2,400 popular business software providers and revealed a highly alarming statistic: 63.6% of vendors that prominently advertise AI capabilities fail to disclose their third-party AI sub-processors in their publicly available legal documentation or Data Processing Agreements (DPAs). This pervasive opacity implies that the majority of healthcare organizations purchasing AI-enabled software may be entirely unaware that they are exposing highly sensitive patient data to downstream AI models and cloud pipelines that they never reviewed, never approved, and possess unknown security postures.
The Cross-Border Intersection: HIPAA and the EU AI Act The geographic location of these sub-processors introduces severe, overlapping regulatory implications, particularly concerning the European Union AI Act. The EU AI Act establishes a comprehensive, extraterritorial framework that enforces strict conformity assessments, risk management protocols, and mandatory post-market monitoring for AI systems classified as "high-risk". In the healthcare sector, AI systems deployed as safety components within regulated medical devices automatically fall under this stringent high-risk classification.
While recent provisional political agreements—part of the "Omnibus VII" simplification package—have proposed delaying the enforcement deadline for general high-risk systems to December 2, 2027, and for medical device safety components to August 2, 2028, the compliance burden remains massive and inevitable. If a U.S.-based AI scribe vendor utilizes a sub-processor located within the EU, or if a U.S. health system processes the data of EU citizens through the scribe, the entire architectural pipeline may fall within the jurisdictional scope of the EU AI Act.
Consequently, healthcare CTOs must demand a complete, transparent, and legally binding sub-processor manifest. This document must detail the specific geographic location of every server, API endpoint, and vector database that touches the clinical audio, the raw transcript, or the generated SOAP note. The vendor must guarantee that all downstream sub-processors are compliant not only with HIPAA but with the impending transparency requirements of the EU AI Act (which remain slated for August 2026 enforcement). This mirrors the broader trend described in Stop Renting Intelligence: Build the AI That Keeps Your Edge, where ownership of the AI stack and its dependencies becomes a strategic necessity.
Pillar 4: Granular Audit Log Architecture and Tamper-Evidence
The HIPAA Security Rule, specifically §164.312(b), explicitly mandates the implementation of robust hardware, software, and procedural mechanisms that record and examine activity in information systems that contain or use electronic protected health information. For clinical AI agents, the volume of data ingestion, the complexity of prompt transformations, and the frequency of API calls require a granularity of logging that traditional enterprise software engineering teams are often unaccustomed to building.
A genuinely compliant AI vendor must be capable of automatically exporting detailed, structured audit logs directly to the healthcare organization's internal Security Information and Event Management (SIEM) system.
The Schema of a Defensible Audit Log: A comprehensive, technically sound audit log entry for an AI scribe must capture highly specific metadata to allow for accurate forensic reconstruction:
event_idand precisetimestampto track the exact millisecond of data interaction.usercontext, including the authenticated User ID, institutional role, and the originating IP address.patientcontext, which must be stored securely utilizing a one-way cryptographic hash (e.g.,sha256:mrn_hash) to avoid the catastrophic mistake of proliferating raw, readable PHI within the log files themselves.agentmetadata, identifying the specific Agent ID, the exact foundational model utilized (e.g., GPT-4o, Claude 3.5 Sonnet, Med-PaLM 2), and the specific model version. This is critical for legal reproducibility; if a clinical note is questioned during a malpractice suit, the organization must know exactly which version of the algorithm generated the text.data_accessedandphi_categories_in_prompt, documenting exactly what structured data the agent queried from the EHR (e.g., medication lists, problem lists) and what categories of PHI were injected into the LLM prompt.
Furthermore, to ensure absolute forensic integrity, these logs must be retained for a minimum of six years in a tamper-evident, Write-Once-Read-Many (WORM) storage architecture. Utilizing services such as AWS CloudTrail with log file validation enabled, writing to an Amazon S3 bucket configured with Object Lock in strict compliance mode, guarantees that neither a malicious external actor, a rogue internal developer, nor the AI system itself possesses the technical capability to alter or delete the forensic history of the patient encounter. Finally, to allow a complete access trail to be reconstructed, the AI agent's audit logs must seamlessly correlate with the EHR's native audit logging by including the EHR session ID within each log entry.
Pillar 5: Incident Response and the Breach Playbook
A credible, mature AI vendor operates under the assumption that a security incident is a statistical inevitability, not an impossibility. Therefore, the vendor vetting process must aggressively interrogate the vendor's incident response maturity and operational readiness.
Beyond negotiating the BAA notification timeline, CTOs should require the vendor to produce an abstracted, redacted copy of their formal Incident Response (IR) playbook. A mature AI vendor will have specific, highly detailed runbooks documenting exactly how their security operations center (SOC) isolates a compromised inference container, how they rapidly halt API connections to the host EHR (e.g., Epic or Oracle Cerner) via immediate FHIR token revocation, and how they conduct post-incident forensic analysis on complex vector databases. This kind of readiness should mirror the resilience patterns used to secure SaaS dependencies against ransomware and outages.
If the vendor cannot produce evidence of annual, comprehensive tabletop exercises simulating a major data exfiltration event, or if they are unable to return a detailed Vendor Risk Management (VRM) questionnaire within 24 to 48 hours, they fundamentally lack the operational maturity required to handle live, critical clinical data. The inability to rapidly articulate their security posture is a glaring red flag indicating internal disorganization.
Certifications That Dictate Trust in 2026
While marketing material and sales presentations are inherently biased, independent, rigorous third-party attestations provide objective, verifiable evidence of a vendor's true security posture. In 2026, the landscape of required cybersecurity certifications has evolved significantly to accommodate the unique, unprecedented risks introduced by generative AI models.
The Baseline: SOC 2 Type II and HITRUST System and Organization Controls (SOC) 2 Type II remains the foundational baseline standard for any cloud service provider. Crucially, healthcare buyers must demand a Type II report, which attests to the operational effectiveness of the vendor's security, availability, and confidentiality controls over an extended, continuous audit period (typically 6 to 12 months). A SOC 2 Type I report—which merely audits the design of controls at a single point in time—is entirely insufficient for an AI scribe handling continuous, high-velocity data streams.
Furthermore, HITRUST CSF certification remains widely regarded as the gold standard specifically within healthcare. Because HITRUST maps controls across HIPAA, NIST, and ISO frameworks, achieving a HITRUST i1 or r2 certification provides a remarkably high degree of confidence in the vendor's enterprise security architecture and maturity.
The New Imperative: ISO/IEC 42001:2023 However, the most critical evolution in vendor vetting is the emergence and widespread adoption of ISO/IEC 42001:2023, the world's first international standard dedicated specifically to Artificial Intelligence Management Systems (AIMS).
While traditional frameworks like ISO 27001 focus broadly on general information security, access control, and data confidentiality, ISO 42001 is purpose-built to address the unique, complex vulnerabilities inherent to artificial intelligence. This framework mandates rigorous controls around algorithmic accountability, ensuring responsible decision-making and understandable AI outcomes. It addresses the robustness and fairness of models, requiring vendors to actively prevent discrimination and mitigate the types of issues frequently discussed in analyses of AI Bias in Healthcare. Furthermore, it demands transparency throughout the full AI lifecycle, from initial design and training data curation to eventual model decommissioning.
Healthcare organizations evaluating vendors in 2026 should view SOC 2 Type II and HITRUST as the absolute minimum barriers to entry, while aggressively prioritizing vendors who have successfully achieved or are actively undergoing formal third-party audits for ISO 42001 certification. This certification serves as definitive proof that the vendor has integrated AI-specific risk management, ethical deployment, and continuous monitoring directly into their corporate governance structure, rather than treating AI safety as a reactive afterthought.
Navigating the Shared-Responsibility Model
A fundamental, often disastrous misconception among clinical leadership and hospital boards is that purchasing a "HIPAA-compliant" AI scribe completely absolves the healthcare organization of ongoing liability. In reality, modern cloud deployments operate on a strict, legally binding shared-responsibility model. The vendor secures the underlying infrastructure, the proprietary algorithms, and the data at rest within their boundaries; however, the healthcare organization remains entirely responsible for securing the application configuration, managing user access, and enforcing patient consent workflows. A perfectly secure, highly certified AI vendor can still cause a catastrophic, multi-million dollar PHI breach if the hospital's internal controls are negligently misconfigured.
Access Control and Configuration Management
The healthcare provider retains ultimate responsibility for identity and access management. This necessitates enforcing strict Multi-Factor Authentication (MFA) for all clinical and administrative personnel accessing the AI tool, executing rigorous, granular Role-Based Access Control (RBAC), and conducting frequent, mandatory access reviews to ensure that departing employees or reassigned staff have their access privileges instantly and permanently revoked.
Furthermore, the technical integration between the AI scribe and the core EHR system must be meticulously configured. For example, when utilizing Cerner FHIR R4 connectivity, the integration should employ industry-standard secure authorization protocols mandated by the ONC 21st Century Cures Act, such as OAuth 2.0 with token-based access control. These API scopes must strictly adhere to the HIPAA principle of minimum necessary, ensuring the AI agent only requests and receives the specific, localized data elements explicitly required to generate the current clinical note, rather than granting the tool unfettered read-access to the entire patient database. This mirrors best practices for enterprise application architecture and secure integration patterns more broadly.
The Operational Burden of Consent Management
The operational, logistical burden of legal compliance falls squarely on the healthcare provider, not the SaaS AI vendor. The deployment of ambient listening tools requires a total, systemic transformation of the clinic's patient consent architecture, extending far beyond traditional intake forms. Providing Virtual Care for Executives or treating highly privacy-sensitive populations requires flawless execution of these consent protocols.
To mitigate severe litigation risks akin to the CIPA/CMIA lawsuits observed in California, healthcare organizations must overhaul their standard operating procedures:
- Implement standardized, heavily documented processes to obtain and formally record patient consent for audio recording prior to every single clinical encounter, treating it with the same gravity as surgical consent.
- Revise comprehensive global treatment consent documents to explicitly, conspicuously detail the use of artificial intelligence, ambient microphones, and external cloud processing for clinical documentation.
- Deploy highly visible, prominent physical signage in waiting areas, hallways, and individual clinical examination rooms notifying patients that ambient AI documentation tools are in active, continuous use.
- Establish frictionless, immediate protocols allowing clinicians to instantly pause recording, delete captured audio, and transition to manual documentation if a patient revokes their consent mid-encounter.
The Strategic Alternative: Self-Hosting vs. Managed AI Scribes
As CTOs meticulously scrutinize the legal risks, sub-processor complexities, opaque data retention policies, and compounding ongoing subscription costs associated with managed SaaS AI scribes, a powerful alternative architectural strategy is gaining significant traction in 2026: self-hosting open-weight models.
For massive Integrated Delivery Networks (IDNs), large academic medical centers, or multi-specialty practices, the fundamental mathematics and risk profiles of self-hosting are becoming increasingly attractive and highly viable. The release of highly capable open-weight foundational models—such as advanced derivatives of Llama 3, Mistral, or Qwen 2.5—allows enterprise organizations to completely bypass third-party APIs. Organizations can download the model weights and execute the inference engines entirely within their own sovereign, on-premises data centers or dedicated, highly controlled private cloud instances (e.g., utilizing Google Cloud A3 Mega VMs featuring NVIDIA H100 GPUs or A3 Ultra VMs with NVIDIA H200 GPUs).
Evaluating Self-Hosting AI Agents for Regulated Enterprises fundamentally changes the security paradigm. By self-hosting, the health system eliminates the need for complex sub-processor BAA negotiations, eliminates the risk of external cloud PHI exfiltration, and guarantees total data sovereignty, solving the EU AI Act cross-border data transfer problem instantly. This echoes the broader argument in Self-Hosting AI Agents: A Guide for Regulated Enterprises that regulated organizations should bring core AI workloads inside their perimeter.
The Economics of Scale: When to Build vs. Buy
The financial decision between a managed SaaS AI scribe and a sovereign, self-hosted deployment hinges entirely on institutional scale. Managed SaaS AI scribes typically operate on a per-seat licensing model, costing between 50 and 200 per provider per month, heavily dependent on total note volume, specific EHR integration depth, and specialty customization requirements.
Consider the financial modeling for a medium-sized enterprise practice with 200 physicians:
- The Managed SaaS Model: Assuming an average negotiated rate of $100 per provider per month, the base subscription cost equals $240,000 annually. When factoring in the initial, often hidden EHR integration and activation fees (10,000–15,000) and external legal counsel review costs for the BAA (1,000–2,000), the first-year total cost of ownership (TCO) easily exceeds $260,000. In this model, the organization remains permanently tethered to the vendor's pricing roadmap, potential future licensing hikes, and rigid data retention policies.
- The Self-Hosted Sovereign Model: By utilizing open-weight models, the organization incurs zero per-user SaaS subscription fees. However, they must lease or purchase dedicated, high-performance GPU compute. Running a highly capable 32-billion parameter model (such as Qwen 2.5 32B, which has demonstrated high efficacy in generating French-language nursing summaries and complex clinical reasoning) requires substantial hardware investment. While direct compute costs may range from 80,000 to 150,000 annually for a dedicated GPU cluster capable of handling the concurrent load, the true, hidden cost lies in specialized human capital. Self-hosting requires an expensive, dedicated internal team of Machine Learning Operations (MLOps) engineers to handle continuous model updates, weight quantization, fine-tuning, complex prompt engineering, and maintaining the secure API integration with the legacy EHR.
For a 200-physician group, the exorbitant personnel costs of maintaining an internal MLOps team generally make the managed SaaS model significantly more economically viable. However, the mathematics invert at an enterprise scale. For a 50-hospital Integrated Delivery System deploying scribes to 5,000 physicians, the annual SaaS costs swell to over $6 million. At that immense scale, self-hosting an open-weight model not only becomes highly cost-effective—yielding millions in annual savings—but provides total, uncompromised control over the organization's proprietary clinical data layer. This is where a broader edge vs. on-prem AI cost and performance analysis becomes essential input to your decision.
The CTO's Vendor Vetting Checklists
To successfully operationalize the highly complex architectural, legal, and regulatory frameworks detailed throughout this report, healthcare technology buyers should utilize the following structured checklists during procurement negotiations. A vendor's inability to provide immediate, concrete, and highly documented answers to these specific technical inquiries constitutes an immediate disqualification.
The Vendor Vetting Framework
| Vetting Category | The Technical Question to Ask the Vendor's CISO | Evidence to Demand During Procurement | Immediate Red Flag Answers |
|---|---|---|---|
| Data Flow & Storage | Where exactly does the ambient audio rest, and what is the technical mechanism for its destruction? | Comprehensive Architecture diagram, formal Data Retention Policy, and detailed encryption key management protocols. | "Audio is stored locally on the clinician's mobile device for quality assurance." or "We use vendor-managed keys exclusively." |
| Training Isolation | Is our PHI or de-identified clinical data used to train your proprietary models or your sub-processor's foundation models? | BAA stipulations explicitly prohibiting secondary use; API contracts with LLM providers proving "Zero Data Retention" endpoints are active. | "We use aggregated, de-identified data to improve the product experience." (If unapproved by hospital policy). |
| Sub-Processors | Who are your 4th-party AI sub-processors, and where are their data centers geographically located? | Complete, exhaustive Sub-Processor Manifest; SOC 2 Type II reports for all listed downstream LLM providers. | Vendor refuses to name the specific foundational LLM they are utilizing, citing "proprietary processing pipelines." |
| Audit Logging | Can your audit logs be seamlessly exported to our SIEM, and what specific metadata granularity do they provide? | Sample JSON audit log schema demonstrating cryptographic hashing of PHI, precise event IDs, and agent model metadata. | "We track basic user logins and the time a note was generated, but we don't log the actual prompt history or data queried." |
| Incident Response | What is your legally binding SLA for breach notification, and what is your internal procedure for isolating a compromised inference container? | BAA featuring a strict 24-to-72 hour notification SLA; abstract of the IR playbook; date of the most recent tabletop exercise. | "We fully comply with HIPAA's standard 60-day breach notification window." |
| Certifications | Do you hold current, independent SOC 2 Type II, HITRUST, or ISO 42001:2023 certifications? | Full, unredacted independent auditor's report (not merely a generic marketing certificate or badge). | Providing a SOC 2 Type I report, or claiming they utilize an AWS data center that is SOC 2 certified (conflating underlying infrastructure with application security). |
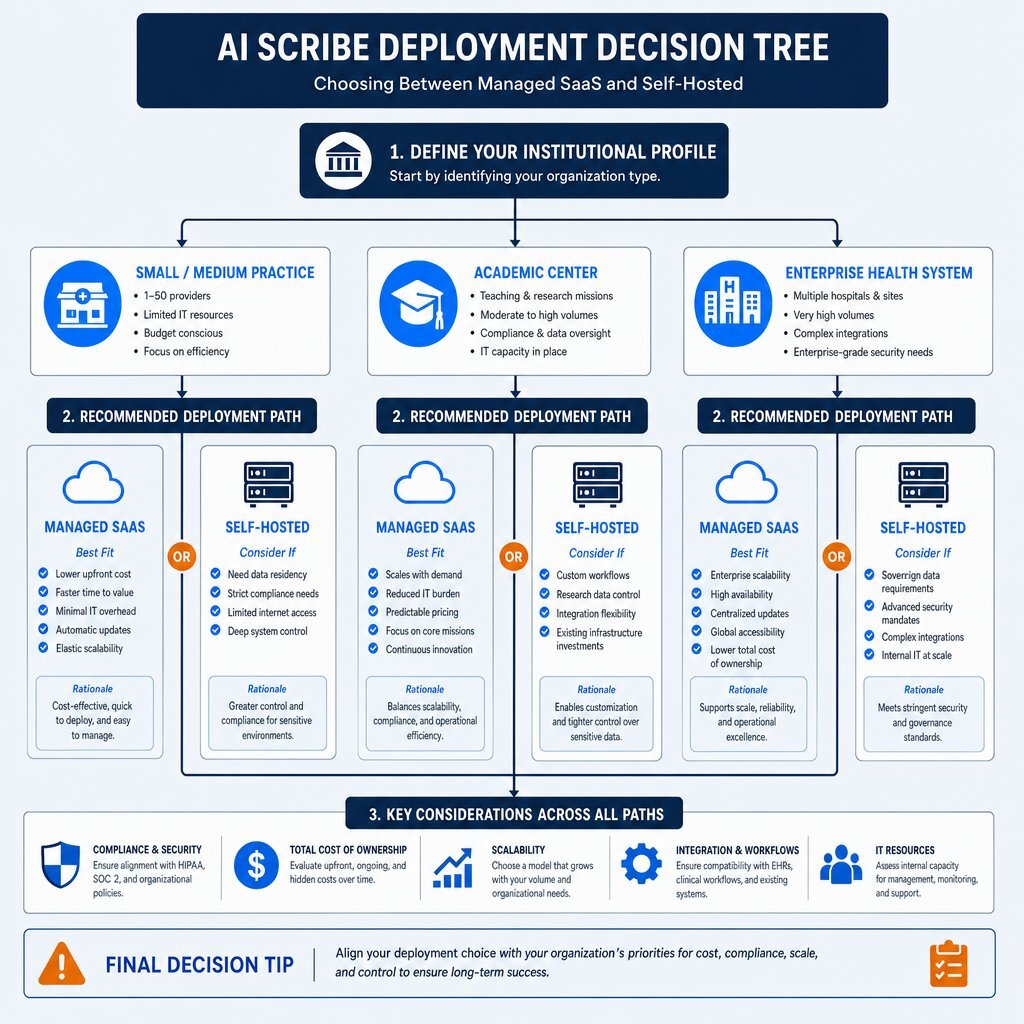
Strategic Deployment Decision Tree
| Organizational Profile | Primary Regulatory Constraints | Recommended Deployment Architecture | Key Rationale |
|---|---|---|---|
| Small/Medium Practice (< 500 Physicians) | Standard HIPAA, State Consent Laws (e.g., CIPA/CMIA) | Managed SaaS (e.g., Suki, Nabla, DeepScribe) | The capital expenditure and MLOps talent required for self-hosting exceed SaaS subscription costs. Focus entirely on BAA negotiation, zero-retention verification, and strict clinic consent workflows. |
| Large Academic Center (High Research Volume) | HIPAA, Institutional Review Board (IRB) restrictions, IP Protection | Hybrid or Self-Hosted | Academic centers cannot risk leaking proprietary research IP or novel clinical methodologies into commercial LLM training corpuses. Open-weight models ensure total data sovereignty for research continuity. |
| Enterprise Health System (> 5,000 Physicians) | HIPAA, EU AI Act (if treating international patients), State Laws | Self-Hosted Sovereign Model (e.g., Llama 3/Qwen on private GPU clusters) | At enterprise scale, SaaS costs become prohibitive ($5M+ annually). Self-hosting provides massive ROI, eliminates 4th-party sub-processor risk, and simplifies complex cross-border compliance mandates. |
Conclusion
The enterprise deployment of AI medical scribes and ambient clinical agents represents one of the most profound, highly necessary operational upgrades to healthcare workflows in the past decade, offering a tangible, empirically proven solution to the devastating epidemic of clinician burnout and administrative overload. However, the architectural reality of streaming live, highly sensitive clinical audio into complex, multi-layered cloud processing pipelines fundamentally alters a healthcare organization's cyber risk profile.
Chief Technology Officers, Chief Information Security Officers, and hospital boards can no longer rely on the superficial, legally meaningless assurance of a basic compliance badge on a vendor's marketing website. The ultimate defense of a health system's operational integrity against devastating OCR audits, aggressive state-level wiretapping class-action lawsuits, and catastrophic, multi-million dollar data breaches relies entirely on rigorous, uncompromising, architecture-first vetting. By demanding transparent data flows, ironclad training isolation, granular forensic audit logging, and highly favorable BAA indemnifications, and by aligning these decisions with a broader portability-first AI strategy for technology and finance leaders, technology leaders can safely harness the transformative power of generative AI. Choosing the right HIPAA compliant AI scribe vendor requires looking far beneath the user interface, ensuring that the underlying architecture fulfills the healthcare industry's paramount mandate: the absolute, uncompromised protection of patient privacy.
About Baytech
At Baytech Consulting, we specialize in guiding businesses through this process, helping you build scalable, efficient, and high-performing software that evolves with your needs. Our MVP first approach helps our clients minimize upfront costs and maximize ROI. Ready to take the next step in your software development journey? Contact us today to learn how we can help you achieve your goals with a phased development approach.
About the Author

Bryan Reynolds is an accomplished technology executive with more than 25 years of experience leading innovation in the software industry. As the CEO and founder of Baytech Consulting, he has built a reputation for delivering custom software solutions that help businesses streamline operations, enhance customer experiences, and drive growth.
Bryan’s expertise spans custom software development, cloud infrastructure, artificial intelligence, and strategic business consulting, making him a trusted advisor and thought leader across a wide range of industries.